Take Another Course
Take Another Course
|
•
Definitions and Overview of IAD
Moisture-associated skin damage, or MASD, is a broad category of skin damage that is related to four categories of problems, including: 1. Skinfolds and sweat, friction, and the presence of bacteria or fungi; 2. Persistent presence of peri-wound exudate--that contains enzymes that damage the skin 3. Peristomal erosion, usually associated with colostomies and ileostomies (and is caused by moisture at the stoma-skin junction) 4. Incontinence-associated dermatitis or IAD. IAD is the most commonly recognized form of MASD.
Definition of IAD So first, let’s define IAD. IAD can be defined as a group of skin conditions that result from excessive amounts of moisture contacting the skin. While IAD is caused by incontinence problems, there are a number of factors that contribute to its development. And perhaps most importantly, complicating factors include the inadequate management of incontinence--which exposes patients to a higher level of risk.
Causes and General Characteristics As for what causes IAD, urinary and/or fecal incontinence that is not well-managed can lead to repeated skin contact with urine or feces. Specifically, IAD is a type of irritant contact dermatitis, which is one of the most common skin problems in incontinent patients. IAD is known by other names, like perineal dermatitis, diaper rash, or moisture or perineal rash. The perianal area is the most common area for IAD. However, the area may be extended if there is greater exposure to incontinence--and how quickly and how often the contaminants are removed—shortening the amount of time the skin has to be in contact with it. The pathophysiology includes several factors, such as the moisture itself, the presence of microorganisms, changes in the skin’s pH, and skin damage from pressure and friction. IAD can be associated with infection, and may happen on both intact and damaged skin areas. As a result, IAD is characterized by inflammation and lesions around the exposed areas. Signs of IAD can include persistent redness and/or skin loss. Other potential characteristics include pain, swelling, and chronic itching and skin-picking (which is also known as ‘excoriation’). These lesions can be complicated by bacterial colonization or fungal infections. While IAD can lead to pressure injuries, these lesions should be differentiated from pressure ulcers and other skin conditions, especially in the genital areas.
Prevalence Knowing the prevalence of IAD can help to understand the relative impact and costs related to the condition. There are a number of prevalence studies that use specific data from databases or a series of studies of specific subgroups, such as patients in the United States in acute care facilities, or patients in long-term and acute care facilities. From these analyses, it is clear that patients with urinary, fecal, and dual incontinence are at greater risk for developing IAD. In a review of data from the United States and Canada, nearly 20% of incontinent patients had documented IAD. Approximately 12% of patients with urinary incontinence and 26% of patients with fecal management systems had documented IAD. And its interesting to see that acute care settings saw a higher prevalence of patients (19%) with IAD compared to long-term care facilities (8.4%).[1] Another retrospective analysis reviewed nearly 16 million patients admitted between 2016 and 2019 and found the prevalence of incontinence at 1.5%--or more than 235,000 patients based on the use of the new ICD-10-CM code for incontinence. Prevalence rates were higher, at 4.1%, for patients 75 years and older. Most incontinence diagnoses were for ‘urinary incontinence only’ (86%) while those ‘fecally incontinent’ (7.3%, and those with ‘dual incontinence’ (6.7%) were lower.[1]
Who gets IAD?
Risk factors that are associated with IAD include any type of incontinence, fecal management systems, higher body weight, lower levels of mobility, longer length of stay, and lower Braden Scale scores. The Braden scale is used for the prediction of pressure injury risk (a lower score indicates a higher risk). Highest risk for the development of IAD may be seen in patients with fecal or dual incontinence. Elderly patients with fragile skin may tend to develop IAD more frequently than other patients. Adding “insult to injury”, patients with IAD were at greater risk for pressure injuries in the sacral area.[2]
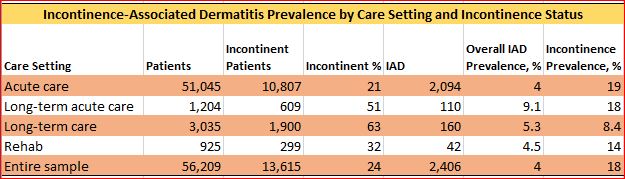
The chart above shows where patients with IAD are predominantly found: In the sample from a study conducted in 2019 of 56,209 retrospectively reviewed patients who were incontinent, those in long-term acute care were the most likely to have IAD (9.1%), followed by long-term care (5.3%), then rehab-based patients (4.5%). The important take-away from this study was nearly 1 in 5 incontinent patients had documented IAD in their charts.[3]
What are the costs? The consequences of IAD include complications to the patient’s health care management, poorer clinical outcomes, and increased health care costs. Health care management hospital costs or “total index hospital costs” for incontinent and IAD patients tend to be 1.2 and 1.3 times higher than for other patients.[4] In general, health care costs tend to be higher, and outcomes tend to be worse, for patients with incontinence who require IAD treatment.
New Diagnostic Code for 2022 Until now, the analysis of prevalence data has been complicated (and probably not very accurate), because an IAD diagnosis was probably not coded. This, no doubt, resulted in an underreporting of the condition. Fortunately, as mentioned earlier, a new billable specific code has been assigned. The 2022 ICD-10-CM diagnosis code L24.A2 in the United States, which became effective in October of 2021, describes irritant contact dermatitis due to fecal, urinary, or dual incontinence.[5]
|