|
Problems with the peristomal skin can be very
uncomfortable for the patient and can make getting a good pouch seal
difficult.
There are many skin complications that can occur. We’ll talk about three
of the more common issues.
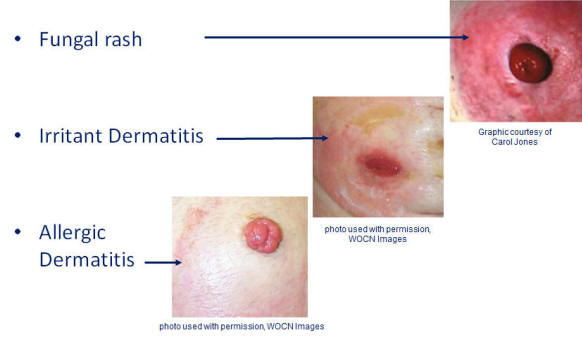
Fungal infections, or candidiasis, are opportunistic
infections that can occur once the peristomal skin has been compromised.
Their host is often old, immunocompromised, or with a history of recent
antibiotic use. These infections thrive in moist, dark, warm places--the
perineum and under the ostomy skin barrier are ideal locations.
Assessment findings include erythema, maceration and papules. Satellite
lesions are found at the periphery. The patient may complain of itching
and burning. Treatment involves making sure the pouch is completely
containing the effluent, keeping it from having contact with the skin.
The skin must be dry prior to the application of the skin barrier.
Before the barrier is applied a topical antifungal powder is liberally
applied. Treatment continues until the skin returns to its intact state.
Irritant dermatitis is usually a result of effluent
coming in contact with the skin as a result of a stoma opening cut too
large or the effluent seeping underneath the skin barrier.
Patients may complain of burning and the resultant skin damage resembles
a chemical burn. This is frequently seen in patients with ileostomies,
due to the caustic nature of the effluent. Skin will be red, moist and
often times denuded (the epidermis is gone and the dermis is exposed
making these areas extremely painful). The areas in question will
resemble those seen in patients with severe urinary incontinence who are
not on skin care regimes, or kids with bad diaper rashes. Treatment
consists of keeping the effluent off the skin by re-evaluating the
current system. A skin barrier powder can also be applied to help dry
the skin.
Allergic Dermatitis is due to a contact sensitivity
reaction to potentially any product that comes in contact with it.
Some clinicians recommend a routine patch test for all patients when a
new product is used. Again, the area will be red and the patient will
experience intense itching, followed by what resembles hives. The area
will become edematous and the skin may crack open. The dermatitis is
confined to the area of skin where the product was applied-so it might
be a square-shaped area of affected skin-exactly the size of the skin
barrier. Management includes discontinuing the offending product, and
initiating the use of antihistamines.
|
|
There are many stoma complications that can occur. Let’s examine four of
them.
Mucocutaneous Separation is a postoperative complication that occurs
when the stoma separates from the skin.
It may be the result of impaired wound healing (secondary to diabetes,
steroid use or infection) or tension related to surgical technique.
Treatment includes filling the separation defect with an absorbent
product and a pouching system that protects the area from effluent. As
the separation heals the stoma needs to be assessed for stenosis
(narrowing of the stoma at the skin or fascial level) or retraction.
Retraction is a condition where the stoma sits below the skin’s surface
level.
The stoma seems to disappear when the patient sits up. Causes of stoma
retraction include post-op weight gain, infection, malnutrition, scars
or adhesions, and mucocutaneous separation. These stomas can cause
effluent to undermine the pouch surface leading to skin breakdown. Using
convex inserts, pouches with built-in convexity, and wearing an ostomy
belt can all help to pop the stoma up in order to get a adequate pouch
seal. Sometimes a surgical revision is warranted.
Prolapse could be thought of as the opposite of retraction, and involves
the bowel telescoping into the stoma.
This area can be susceptible to trauma, challenging to pouch, and is
sometimes very offensive to the patient. Causes may include pulling the
colostomy through an abdominal incision, using a large fascial opening
in the abdominal wall, or the presence of an obstruction when the
colostomy was created. A careful selection of products that are flexible
can avoid this type of trauma. By carefully measuring the stoma opening
when the patient is standing, since that is usually when the prolapse
will be at it’s biggest, will help to ensure proper stoma placement,
tension and positioning. Patients can be taught to apply the pouch after
they have gently applied pressure or even ice for several minutes in
order to reduce its size.
There
are a variety of challenges that should be avoided. Pouching a patient
with two stomas, pouching a stoma that has a surgical wound dehiscence,
pouching in patients receiving irradiation treatment, pouching morbidly
obese patients, stoma necrosis and parastomal hernia are all challenges
that are seen and overcome using proper product selection and good
technique. And if you’re lucky, you’ll have a certified ostomy nurse
available who lives for these very challenges! |
 Instructions
Instructions Take Another Course
Take Another Course